Introduction
Introduction
Chronic Disease Management (CDM) in General Practice involves early identification of chronic disease, appropriate primary and secondary prevention, and evidence based management. Nurse-Doctor teams have a key role to play in these areas of chronic disease in the community, as General Practice is usually the first point of contact in the health system.
PAT offers a number of innovations:
- It offers a work force solution based on the concept of the Patient-Nurse-Doctor team. The patient does about 40% of the questions in each clinic and their choices in these questions determine the treatment plan offered.
- It allows the option of converting the waiting room to a “virtual office” because patients can do their touch-screen responses there. This saves consulting room space.
- It saves doctor time by automatically generating a relevant GPMP. The only problems that appear in the plan are when the question answered by the doctor or patient requires ongoing management.
- Education is supplied in a small amount in each patient question. This enables the patient to understand both why the question is asked and to increase their understanding in short bursts.
- Evidence based medicine from the relevant guideline is similarly supplied in a small amount in each doctor question.
- A comprehensive algorithmic approach in the doctor questions ensures an easy use of guideline recommendations.
GP Management Plans (GPMPs)
A GP Management Plan (Item 721) may be completed by the patient’s usual GP for any chronic condition. A chronic condition is one that is likely to last 6 months or longer or is terminal. The minimum time to repeat the GPMP is 12 months unless the patient’s condition changes significantly.
Team Care Arrangements
A Team Care Arrangement (Item 723) can be completed after an Item 721 and this entitles the patient to 5 subsidised allied health visits in a 12-month period. PAT automatically generates the Team Care Arrangement (TCA) form for allied health refferals.
Annual cycles of care
- An Asthma cycle of care may be completed for moderate to severe asthmatics once in a 12 month period (items 2546, 2552, 2558 which then trigger a SIP of $100).
- A Diabetes cycle of care may be completed for all diabetics between 11 and 13 months each year (items 2517, 2521, 2525 which then trigger a SIP of $40).
- Health Assessments such as the age 75 and 45 to 49 assessments for patients who are at risk of developing a chronic disease (items 701, 703, 705, 707).
The PAT tool will greatly assist with these areas and item numbers, and consists of 3 main sections:
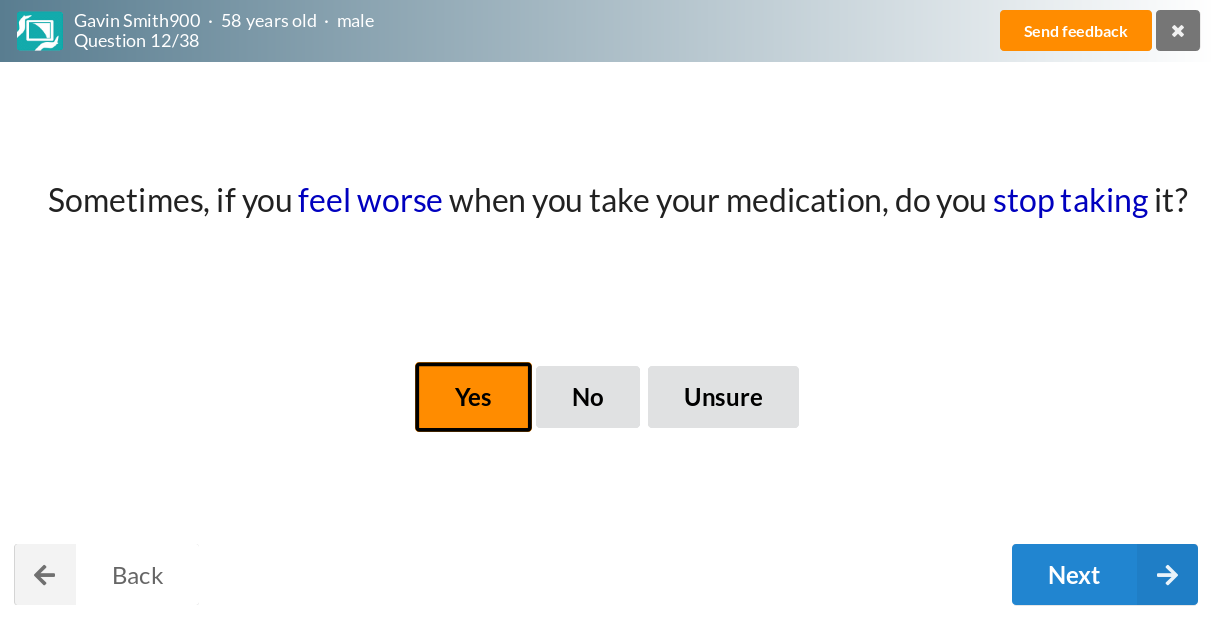
1. Patient section
Patients, either with the aid of a nurse, answer a questionnaire on a touch-screen device and get interactive education based on their answers. The education includes motivational interviewing for smoking, losing weight & exercising. Answers to specific questions are used by the software to customise the Management Plan.
2. Nurse section
The Nurse Section is a checklist of tasks needed to be performed before the patient sees the doctor. Added to the patient section answers it provides the doctor with a comprehensive starting point.

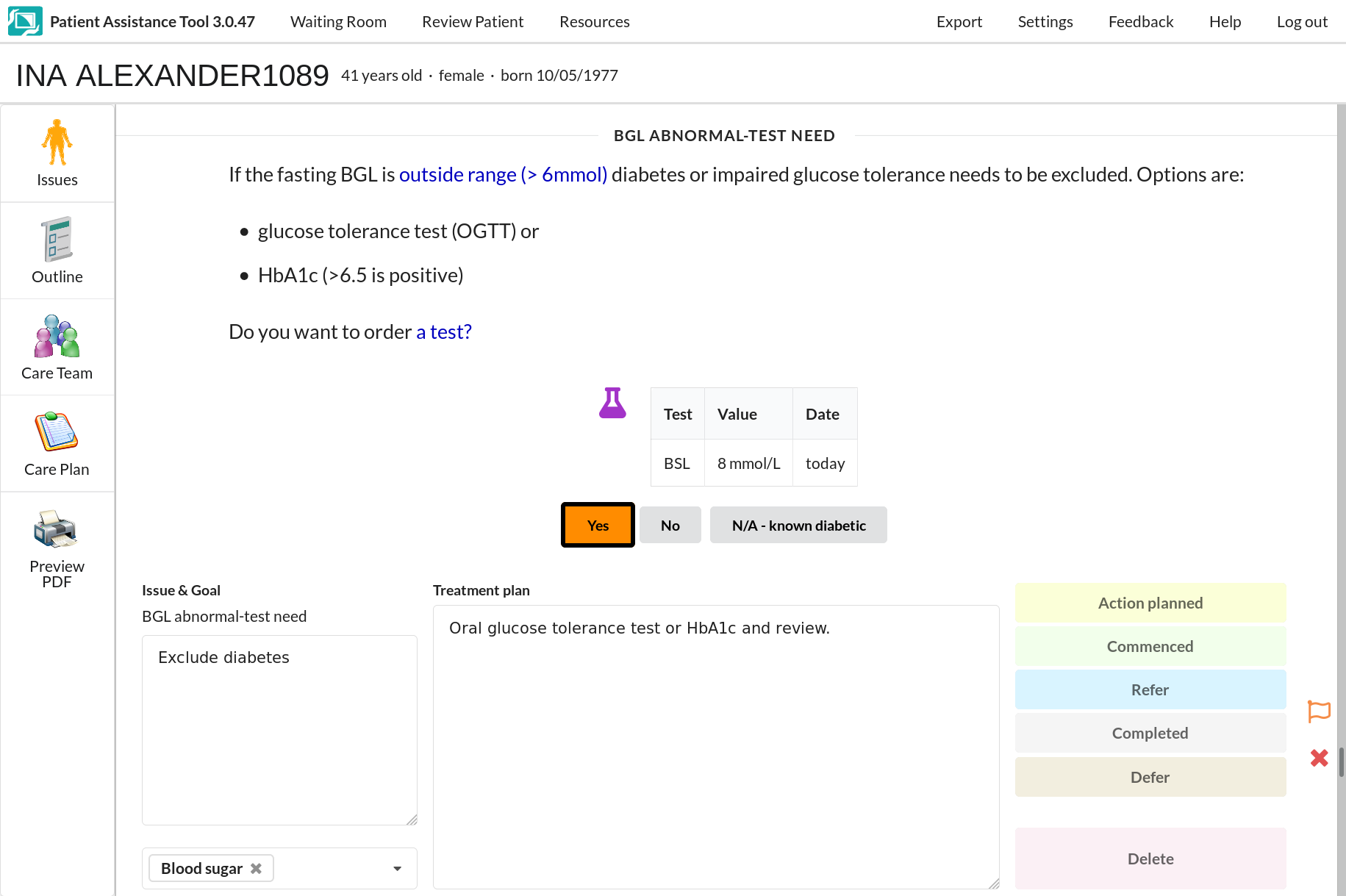
3. Doctor section
The doctor completes a number of questions that include relevant pathology results, data entered by the nurse and links to evidence-based guidelines. A management plan is incrementally generated semi-automatically and edited to suit the person. The management plan combines relevant data entered by the patient and doctor.